


1Department of Medicine, Universitat Autònoma de Barcelona, 2Department of Dermatology, 3Department of Pathology and 4Molecular Diagnostics Laboratory, Department of Pathology, Hospital del Mar–Parc de Salut Mar, and 5Methodological and biostatistical advisory service, IMIM (Hospital del Mar Medical Research Institute), Barcelona, Spain
#These authors contributed equally to this work.
BIOMED-2 Concerted Action BMH4-CT98-3936 (BIOMED-2) PCR protocols are an important diagnostic tool in the evaluation of cutaneous lymphomas. The aim of this study was to assess the diagnostic value of the genotyping results obtained by these techniques in daily clinical practice. A total of 360 paraffin-embedded skin samples were retrospectively reviewed from 114 cutaneous T-cell lymphomas and 35 cutaneous B-cell lymphomas. A total of 249 biopsies from 180 patients with benign lymphoid infiltrates served as controls. T-cell receptor and immunoglobulin gene rearrangements were assessed using the BIOMED-2 method. A combined T-cell receptor gamma and beta assay approach reliably distinguished cutaneous T-cell lymphomas from benign skin T-cell infiltrates (sensitivity 89.4%; specificity 81.5%). Analysis of complete immunoglobulin heavy chain rearrangements also differentiated cutaneous B-cell lymphomas from benign B-cell infiltrates (sensitivity 85.7%; specificity 82.4%). In conclusion, the full BIOMED-2 protocol is a useful aid combined with clinical, histological and immunophenotypical findings for assessment of lymphoid clonality in skin lymphoid proliferations.
Key words: BIOMED-2; clonality; cutaneous B-cell lymphoma; cutaneous T-cell lymphoma; multiplex polymerase chain reaction; T-cell receptor genes; immunoglobulin genes.
Accepted May 5, 2021; Epub ahead of print May 6, 2021
Acta Derm Venereol 2021; 101: adv00460.
doi: 10.2340/00015555-3828
Corr: Daniel López Aventín, Department of Dermatology, Hospital del Mar, Universitat Autònoma de Barcelona, pg. Marítim 25-29, ES-08003 Barcelona, Catalonia, Spain. E-mail: dlopezaventin@parcdesalutmar.cat
Diagnosis of cutaneous lymphomas is often challenging due to its clinical, histopathological and immunophenotypical overlap with a broad spectrum of benign lymphoid infiltrates. Clonality evaluation using the BIOMED-2 Concerted Action BMH4-CT98-3936 (BIOMED-2) method has been useful in certain cases. However, the relevance of the different clonality assays, performed individually or combined, in benign and malignant skin lymphoid proliferations in real-life clinical practice has scarcely been explored. This study found that combined T-cell receptor gamma and beta analysis increased clonal detection sensitivity in cutaneous T-cell lymphomas. Conversely, additional assays to the routine complete immunoglobulin heavy chain assessment were helpful in selected controversial B-cell infiltrates.
Primary cutaneous lymphomas (PCL) are a heterogeneous group of T- and B-cell malignant lymphoproliferative disorders presenting in the skin, with no evidence of extracutaneous disease at the time of diagnosis. Cutaneous T-cell lymphomas (CTCLs) represent 75–80% of all PCL, whereas cutaneous B-cell lymphomas (CBCLs) account for approximately 20–25% (1, 2). Diagnosis of PCL is based on the accurate integration of clinical presentation, histopathological findings, immunophenotypical criteria and molecular data. This comprehensive correlation of results is of paramount importance in cases without conclusive clinicopathological features, including early-stage mycosis fungoides (MF), and CBCLs with indolent course, in which distinguishing between reactive inflammatory and neoplastic cutaneous lymphoid infiltrates may be extremely difficult (3–6).
T-cell receptor (TCR)/immunoglobulin (Ig) clonality testing is performed on cases of suspected PCL as an ancillary technique to provide additional evidence for diagnosis (7–9). Although the presence of monoclonality is a supportive feature of malignancy, a clonal population could also be demonstrated in some well-recognized inflammatory skin conditions (3, 6, 9–13).
PCR protocols are the gold standard techniques for molecular clonality studies. However, the different PCR-based clonality analyses displayed relevant differences in the methodological procedures (various oligonucleotide primers and diverse detection methods for amplified PCR products) and the results obtained from different studies could hardly be compared (14). In 2003, a European collaborative work developed a uniform and standardized protocol, BIOMED-2 Concerted Action BMH4-CT98-3936 (BIOMED-2), which facilitates the detection of clonal lymphocyte populations of any origin, including the skin (7, 15). BIOMED-2 gained popularity over other PCR methods because it covers almost all possible TCR/Ig gene rearrangements (GR) and commercial availability (InVivoScribe, San Diego, CA, USA) (5, 7, 14, 15). Nonetheless, most of the previous studies in PCL were restricted to specific diagnoses, predominantly MF, and often did not evaluate TCR beta (TCRB) or incomplete Ig heavy chain (IGH) (DH-JH) and Ig kappa (IGK) GR as targets for clonality tests in CTCLs and CBCLs, respectively.
The aim of the current study was to investigate the value of performing most of the multiplex PCR assays available from the standardized BIOMED-2 method for distinguishing CTCLs and CBCLs from benign cutaneous lymphoid infiltrates (BCLI) in real-life clinical practice. A further aim was to evaluate the practical usefulness of this method for clonality assessment in peripheral blood (PB) samples from patients diagnosed with CTCLs, CBCLs and BCLI.
Case selection
A total of 360 skin biopsies were retrospectively reviewed from 149 patients evaluated in the Department of Dermatology, Hospital del Mar in Barcelona, from January 2004 to December 2014 and diagnosed according to the 2018 update of the World Health Organization–European Organization for Research and Treatment of Cancer (WHO-EORTC) classification for PCL (2). Specific diagnoses given in the 114 patients with CTCLs were as follows: MF (n = 47), folliculotropic MF (n = 7), pagetoid reticulosis (n = 1), Sézary syndrome (SS) (n = 10), lymphomatoid papulosis (LyP) (n = 17), primary cutaneous anaplastic large cell lymphoma (C-ALCL) (n = 3), subcutaneous panniculitis-like T-cell lymphoma (n = 1), extranodal NK/T-cell lymphoma, nasal type (ENKL) (n = 2), primary cutaneous aggressive epidermotropic CD8+ cytotoxic T-cell lymphoma (n = 1), primary cutaneous CD4+ small/medium T-cell lymphoproliferative disorder (n = 8), and primary cutaneous peripheral T-cell lymphoma, not otherwise specified (PTCL, NOS) (n = 6). In addition, 11 patients had both MF and a primary cutaneous CD30+ T-cell lymphoproliferative disorder (10 LyP and 1 C-ALCL). Fifty (76%) of 66 patients with MF were classified as early MF (stages IA–IIA) based on the International Society for Cutaneous Lymphoma algorithm (scoring 4–6 points) and a negative staging work-up (16). On the other hand, 35 patients diagnosed with CBCLs were classified as: primary cutaneous marginal zone lymphoma (PCMZL) (n = 21), primary cutaneous follicle center lymphoma (PCFCL) (n = 12), and primary cutaneous large B-cell lymphoma, leg type (PCDLBCL, LT) (n = 2).
A total of 249 biopsies from 180 patients with BCLI were included as controls. These patients had the following most common diagnoses: 31 digitate dermatosis or small-plaque parapsoriasis, 30 dermatitis not otherwise specified, 19 reactive cutaneous lymphoid hyperplasias, 11 pityriasis lichenoides, 10 pigmented purpuric dermatoses, 9 lichenoid dermatoses, 8 erythrodermic inflammatory dermatoses, 7 adult atopic dermatitis, 5 cutaneous lupus erythematosus, 5 cutaneous adverse drug reactions and 3 arthropod bite reaction. These patients were chosen because their biopsies had prominent lymphocytic infiltrates and clinicopathologically were suspicious of PCL.
From all the 329 patients formalin-fixed paraffin-embedded (FFPE) skin biopsies were studied. A total of 142 patients had 2 or more skin biopsies performed at different time-points (n = 129) or simultaneously at more than one site (n = 13). In 179 cases, PB samples were also analysed. The study was approved by the local Clinical Research Ethics Committee (record number 2016/6719/I).
Clonality analysis
Genomic DNA was extracted from 2 15-μm sections of representative FFPE skin biopsies using the QIAamp DNA MiniKit (Qiagen GmbH, Hilden, Germany) following the manufacturer’s instructions. The quality of each DNA sample was confirmed by BIOMED-2 control PCR (15). Genomic DNA from peripheral blood mononuclear cells was isolated with Genovision M48 (Qiagen).
Clonality was assessed using the BIOMED-2 primer sets for TCR gamma (TCRG) and TCRB in cases suspicious of CTCLs, and B-cell clonality was analysed using IGH (complete and incomplete GR) and IGK assays, following PCR conditions and analysis as described (15). All cases were tested in duplicate to avoid pseudoclonality. A sample was considered monoclonal if the height of 1 or 2 prominent peaks within the valid range was greater than 2-fold the polyclonal/background signal and the same peak was identified in the duplicate runs (15, 17).
Statistical analysis
Data were summarized using frequencies, percentages, medians and ranges. To evaluate the diagnostic value of the different BIOMED-2 PCR clonality assays, CTCLs, MF, early MF or CBCLs were chosen as the disease to be diagnosed and BCLI were considered as controls. Clinicopathological correlation and data from the follow-up were established as the gold standard for diagnosis. The detection of monoclonality or a clonal pattern in a polyclonal background were considered as a positive test and polyclonality, oligoclonality or pseudoclonality as a negative result. Combination of various clonality assays were considered positive (clonal) if any test was monoclonal. Sensitivity, specificity, positive predictive value, negative predictive value and their 95% confidence intervals (95% CI) were calculated to define the utility of the different diagnostic tests and compared applying the “DTComPair” package from R software (18). A difference was considered statistically significant when p-value < 0.05. Analyses were performed using STATA SE version 15.1 (StataCorp, College Station, TX, USA) and R software version 3.6.2 (R Foundation for Statistical Computing, Vienna, Austria).
The clinical characteristics of the patients included in the present study are summarized in Table SI.
Cutaneous T-cell lymphomas
Of the 114 cases of CTCLs, there were 42 females and 72 males with a median age at diagnosis of 54 years (range 8–85 years). In 102 (89.5%) patients a monoclonal TCR GR (TCRG and/or TCRB) was observed in FFPE skin biopsies. The majority of cases of MF (61/66, 92.4%) showed a clonal pattern, including those cases with early MF (45/50, 90%). In fact, only 2 patients diagnosed of MF with stage IA (T1a) and 3 with stage IB (T2b) disclosed negative results. The remaining 7 CTCLs with polyclonal pattern were LyP type A. An identical clone was detected in 54/63 (85.7%) patients with multiple cutaneous biopsies. Most of the patients who had both MF and LyP (83%) shared identical monoclonal TCR GR, suggesting a common origin between these distinctive clinicopathological entities.
The 10 patients with SS showed 2,768/mm3 median circulating Sézary cells (range 517–14,931). By flow cytometry, median CD4+CD7– and CD4+CD26– subsets were 2,757 cells/mm3 (ranges 854–20,313 and 1,340–20,750, respectively). A blood T-cell clone was identified by TCRG GR analysis in all cases examined. In addition, cutaneous monoclonality was demonstrated by both tests (TCRG and TCRB) in 8 out of 10 cases.
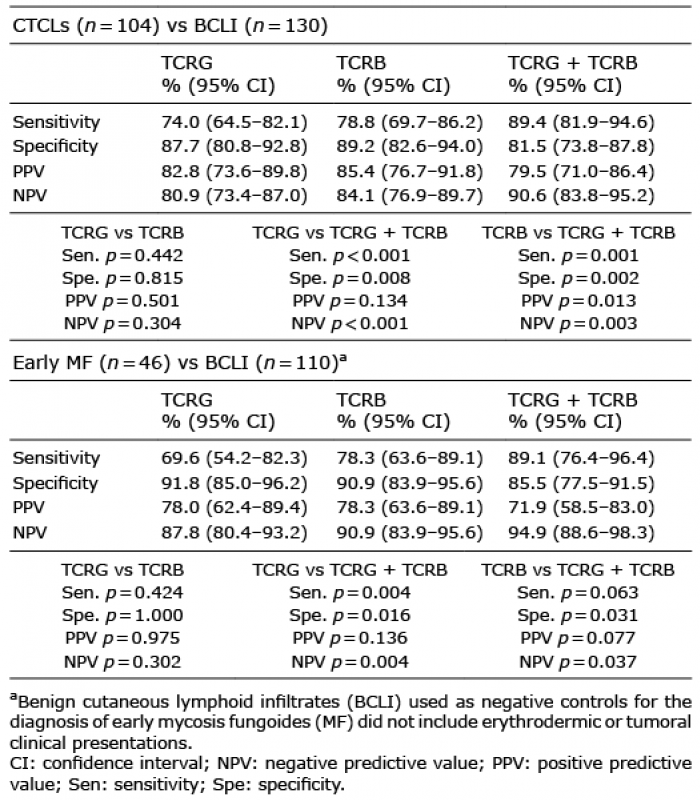
Analysis of TCRB was slightly more sensitive (78.8%) than TCRG testing (74%) in the diagnosis of CTCLs when evaluated as individual assays. Of note, this difference in sensitivity was higher when considering early MF (TCRB: 78.3% vs TCRG: 69.6%). As single tests, specificity rates were 87.7% and 89.2% using TCRG and TCRB clonality tests, respectively. Combined use of both tests was significantly more sensitive in diagnosing CTCLs (89.4%) and early MF (89.1%) than TCRG alone. Although the concordance rate in the results of both assays was 74% in CTCLs and 69.6% in early MF cases, there were patients in which monoclonality was only detected by one of the tests, improving the diagnosis rate with the combined PCR assays strategy. Conversely, combining the TCRG and TCRB tests also significantly diminished diagnostic specificity as more cases of BCLI demonstrated clonality by either test. The obtained results of clonality detection in cutaneous biopsies from patients with CTCLs, early MF and BCLI are shown in Table I and Fig. 1.
Table I. Sensitivity, specificity, positive predictive value and negative predictive value of T-cell receptor gamma (TCRG) and T-cell receptor beta (TCRB) BIOMED-2 Concerted Action BMH4-CT98-3936 (BIOMED-2) PCR in cases of cutaneous T-cell lymphomas (CTCLs) and early MF
Fig. 1. Concordance between T-cell receptor gamma (TCRG) and T-cell receptor beta (TCRB) BIOMED-2 Concerted Action BMH4-CT98-3936 (BIOMED-2) assays in skin biopsies of malignant and benign T-cell proliferations. CTCLs: cutaneous T-cell lymphomas; MF: mycosis fungoides; SS: Sézary syndrome.
A T-cell clone was detected in blood samples from 59 out of 95 (62%) patients with CTCL. Nevertheless, detection of an identical clone in the PB and skin occurred only in 15 of those 59 cases. Most of the patients who showed the same dominant cutaneous and blood T-cell clone were, as expected, SS (n = 8), but also 5 cases of MF (stages IA, IIA and IVA2) and 1 each of PTCL, NOS and ENKL. In contrast, non-related circulating T-cell clones were observed in almost half of patients with MF (53.3%) and early MF (45.5%). This finding was significantly more common in patients aged 60 years or older (median age 62 vs 49 years, p = 0.014). The results of clonality detection in patients with PB and skin biopsy specimens are depicted in Fig. 2. Median follow-up in patients with CTCL was 75.2 months (range 1.2–311.2 months).
Fig. 2. Results of clonality detection in patients with BIOMED-2 PCR evaluation in the skin and peripheral blood samples. CBCLs: cutaneous B-cell lymphomas; CD30+ LPDs: primary cutaneous CD30+ lymphoproliferative disorders; CTCLs: cutaneous T-cell lymphomas; MF: mycosis fungoides; PCR: polymerase chain reaction; SS: Sézary syndrome.
Cutaneous B-cell lymphomas
Of the 35 patients with CBCLs, 33 had a diagnosis of indolent type lymphoma (PCMZL or PCFCL). There were 18 females and 17 males, with a median age at diagnosis of 60 years (range 21–97 years). Complete IGH (VH-JH) GR assessment alone detected monoclonality in 31 (88.6%) of the 35 CBCLs. Of the 3 segments analysed to evaluate IGH (VH-JH) GR, VH framework region (FR)1-JH segment yielded the highest clonal outcome (67.7%), followed by VH FR2-JH (55.9%) and VH FR3-JH (47.1%). Only 4 patients, 3 PCMZL and 1 PCDLBCL, LT exhibited non-clonal results in the IGH (VH-JH) assessment. However, the addition of IGK and incomplete IGH (DH-JH) tests also allowed a clonal GR to be identified in those 4 cases. The results of clonality detection in patients with CBCLs and BCLI are shown in Table II. In patients with multiple skin samples, 15 of 17 (88.2%) had identical B-cell clones. Conversely, 2 patients with PCFCL revealed clonal, but different, IGK and IGH VH FR1-JH / IGH VH FR2-JH GR, respectively. Both cases achieved complete response and were alive without disease at the end of the follow-up. Median follow-up time in patients with CBCLs was 81.9 months (range 1.8–376.8 months). Finally, evaluation of B-cell clonality in PB samples showed a dominant circulating clonal population, different from the dominant cutaneous clone, in 6 (21.4%) out of 28 patients with CBCLs analysed (Fig. 2).
Benign cutaneous lymphoid infiltrates
A total of 180 patients with BCLI encompassing a wide variety of inflammatory entities were included in this study. There were 65 females and 115 males with an age range of 0–92 years (median age 62 years). Thirty-six (20%) patients exhibited a monoclonal result in 1 of the cutaneous biopsies (Table SII). In 11/12 (92%) cases with multiple skin samples, an identical clonal population was not detected. The exception was a 61-year-old male who presented identical TCRG GR in both biopsies performed 14 months apart and consistent with pityriasis lichenoides.
Thirty (53.6%) out of 56 patients revealed a monoclonal GR, mostly with the TCRG assay, in PB samples. Interestingly, only 2 patients had identical circulating and cutaneous T-cell clones (Fig. 2). One of these patients presented an idiopathic erythroderma without morphological or flow cytometric blood involvement who progressed to SS after 10.2 years of follow-up. The second case was a male diagnosed with pityriasis lichenoides who died of lung carcinoma after 7.2 years of follow-up.
The diagnosis of PCL is occasionally challenging, due to its clinical, histopathological and immunophenotypical overlap with a wide spectrum of benign cutaneous lymphoid proliferations. Using the standardized BIOMED-2 PCR protocol in CTCLs this study observed that the global sensitivity of clonal detection was enhanced when evaluating both TCRB and TCRG GR (from 74% with TCRG alone to 89.4% with TCRG and TCRB). In the current series, analysis of TCRB allowed the detection of monoclonality in almost 60% of cases in which negative results with TCRG assessment had been obtained. Although TCRG PCR-based analysis is the most widely used test due to the restricted repertoire of V and J segments that can be covered by a reduced number of PCR primers, the limited combinatorial and junctional diversity of TCRG GR may complicate the distinction between monoclonal and polyclonal patterns in some cases (15, 19). Recently, Schachter et al. (20) reported a higher sensitivity rate of TCRB (83%) compared with TCRG (43%) in early MF. In the current study cohort of patients, TCRB was also more sensitive than TCRG in such cases, but the difference was statistically non-significant. A few studies have previously suggested performing TCRG and TCRB tests in tandem in order to improve the diagnosis rate (8, 20). In our experience, the combined use of both tests increased the cost by 70 € for each sample compared with the TCRG alone (50 €). The negative counterpart of this strategy was a diminution of specificity from 91.8% with TCRG alone to 85.5% with the combined usage of TCRG and TCRB in distinguishing early MF from inflammatory dermatoses. Evaluation of multiple skin biopsies from the same patient performed either at different time-points or at more than one location could help to counteract the reduction in diagnostic specificity. Indeed, identical clones were detected in 85.7% of patients with CTCLs. In contrast, the identification of the same clone in more than 1 skin biopsy was exceedingly rare among patients with BCLI. These observations are in agreement with Thurber et al. (21), who proposed that the presence of identical clones in 2 distinct biopsies was highly suggestive of MF.
On the other hand, PCMZL and PCFCL represent the majority of CBCLs and are often difficult to distinguish from reactive cutaneous lymphoid hyperplasias (CLH) (22). Previous studies have investigated the role of clonality analysis by PCR, achieving variable detection frequencies from 27% to 95% (5, 9, 23–25). In the current series, a high percentage of CBCLs (88.6%) showed monoclonality by complete IGH (VH-JH) GR assessment. Moreover, additional analysis of IGK and incomplete IGH (DH-JH) GR demonstrated a monoclonal result only in isolated cases of PCMZL and PCDLBCL, LT formerly interpreted as polyclonal. Somatic hypermutations of the IGH gene in some CBCLs may hamper amplification of the VH-JH target and stress the relevance of IGK or incomplete IGH (DH-JH) GR, as these are assumed to be free of somatic hypermutations (9, 15). Nevertheless, the addition of IGK and incomplete IGH (DH-JH) analysis raised the economic cost by 100 € for each sample compared with IGH (VH-JH) assessment alone (70 €).
In addition, when IGH and IGK assays were performed in combination, a clone was detected in 26.7% of patients with CLH evaluated. The diagnosis of CLH was established based on clinicopathological correlation and achievement of complete response spontaneously or after minimal local therapy. Thus, the demonstration of monoclonal IGH or IGK GR by BIOMED-2 PCR protocol is a useful aid in the diagnosis of CBCLs, always taking into account the clinical presentation, histological and immunophenotypical features. In addition, the option of a clonal CLH within a continuum spectrum of B-cell lymphoproliferative disorders should also be considered (26).
Another issue evaluated in the current study was the utility of T-cell and B-cell clonality analysis in PB samples. Circulating dominant clones were detected in 62% of CTCLs, 21.4% of CBCLs and 53.6% of BCLI. Muche et al. (27) and Delfau-Larue et al. (28) detected circulating T-cell clones in 65.2% and 51.3% of their patients with CTCLs, respectively. However, the majority of blood clones identified in the current study cohort were not related to the cutaneous clones and may correspond to clonal T-cell expansions in elderly individuals (27–29). The exceptions of this observation were, as expected, patients with SS and isolated cases of MF, PTCL, NOS and ENKL. Remarkably, there were 8 patients with SS but also one patient with an idiopathic erythroderma who progressed to SS after 10.2 years of follow-up. Such cases emphasized the importance of clonality investigation in PB and skin samples in erythrodermic patients. Long-term close follow-up in all cases with identical circulating and cutaneous T-cell clones is recommended (30, 31).
Identical T-cell clones in skin and blood were identified in 4 out of 44 (9.1%) cases of early MF (stages IA-IIA). Intriguingly, the same result (6/66, 9.1%) was described by Delfau-Larue et al. using a non-BIOMED-2 TCRG PCR technique in one of the largest studies aiming to determine the frequency and diagnostic value of circulating T-cell clones in patients with a clinical suspicion of cutaneous lymphoma (28). Other authors also found identical circulating clonal T cells to those in lesional skin even in the early stages of MF (27, 29, 32–34). The proposed pathogenic mechanisms for these findings have included a stage-independent physiological recirculation of the neoplastic cells via the PB to the skin and, more recently, that cutaneous lesions of MF are composed by consecutive seeding of clonotypically heterogeneous neoplastic T-cell clones from the blood to the skin (27, 35). Circulating clonal T cells were found in 81.3% of our patients diagnosed with advanced MF (stages IIB–IVB), but only 6.3% of these cases showed identical T cell clone in skin and blood. The prognostic significance of such a low level of blood involvement, only detected by molecular means, in MF has been contradictory and is probably going to be clarified by the ongoing PROspective Cutaneous Lymphoma International Prognostic Index Study (PROCLIPI) (36).
On the other hand, our experience in B-cell clonality analysis in PB samples from patients diagnosed with CBCLs, mostly PCMZL and PCFCL, confirms the lack of clinical relevance. No cases with an identical skin and blood B-cell clone were identified. Legrand et al. (37) recently found an identical blood and skin IGH clone in 6.9% of 58 patients with PCMZL, and concluded that assessing blood B-cell clonality has no clinical relevance for therapeutic options and prognosis.
This study has some limitations. It is a retrospective analysis of a large series of patients selected from a single institution. Furthermore, in cutaneous B-cell lymphoid infiltrates, the observed results were not compared with those obtained with other ancillary techniques, such as immunohistochemistry or in situ hybridization to evaluate for light chain restriction. In addition, the combined use of different/multiple PCR tests increases the economic cost of the technique and may be a potential drawback, albeit to a lesser extent than some promising and more sophisticated technologies, such as TCR gene high-throughput sequencing (HTS) analysis (38–44). Although HTS might, in the future, become the gold standard for routine clonality analysis in CTCLs, one recent study using TCRB sequencing in skin obtained a sensitivity of 68% and specificity of 100% for distinguishing CTCLs from reactive conditions, rates that are not so disparate from what we found by BIOMED-2 TCRB PCR assay (sensitivity 78.8% and specificity 89.2%) (41). Other encouraging studies on TCR sequencing in CTCLs only used BIOMED-2 TCRG primers and protocols for comparison, missing the enhanced value of combining TCRG and TCRB PCR methods (38, 39).
Therefore, an individualized approach seems advisable when assessing T-cell or B-cell clonality in patients with non-conclusive clinicopathological, immunophenotypical and evolutive features. In CBCLs, complete IGH (VH-JH) GR assessment detected B-cell clonality in nearly 90% of patients, suggesting that additional IGK and incomplete IGH (DH-JH) assays are helpful only in controversial cases. In contrast, the combined BIOMED-2 TCRG and TCRB assays are more useful than the most-often performed individual TCRG test.
In conclusion, BIOMED-2 PCR protocol has wide availability and produces satisfactory results, and is thus a useful tool in routine clinical practice. The combined approach of multiplex PCR assays available from the standardized BIOMED-2 method increases the sensitivity rate of clonality detection.
This study was supported in part by grants from Instituto de Salud Carlos III (ISCIII) PT17/0015/0011 and Xarxa de Banc de Tumors de Catalunya.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize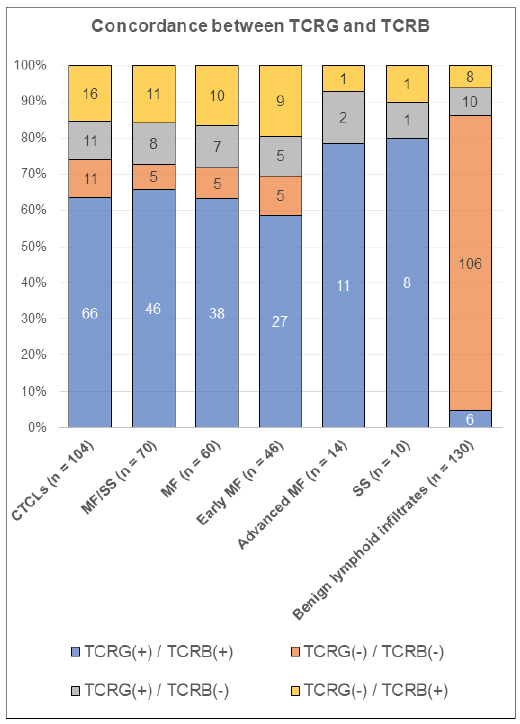 Click to show fullsize
Click to show fullsize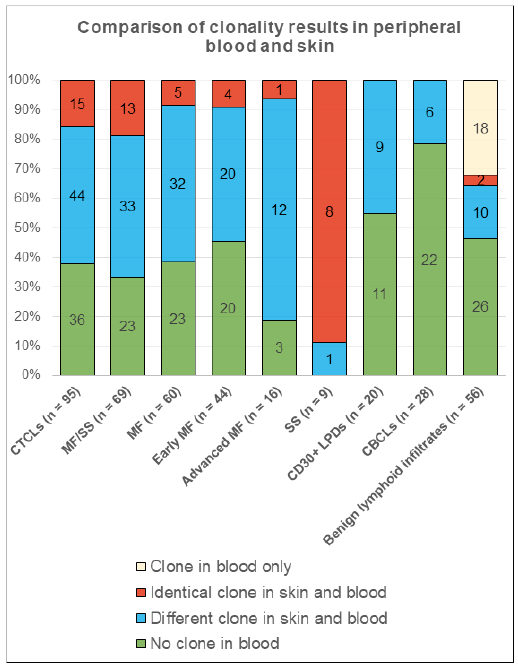 Click to show fullsize
Click to show fullsize